Zofran
"Order generic zofran, medicine jar paul mccartney."
By: Tristram Dan Bahnson, MD
- Professor of Medicine

https://medicine.duke.edu/faculty/tristram-dan-bahnson-md
In the early 1950s medications in carry on luggage discount zofran online visa, industrial research in the United Kingdom attempting to medicine 1920s buy cheap zofran 8mg online develop more effective pesticides led to medicine 44175 order zofran toronto the discovery of the nerve agent amiton, which was used for a short time in agriculture, but was then withdrawn because of its high mammalian 14 | C h a p t e r 1 – I n t r o d u c t i o n a n d h i s t o r i c a l o v e r v i e w toxicity. It was subsequently discovered that replacing one of the phosphorus-alkoxy bonds in amiton with a phosphorus-methyl bond increased the toxicity by at least a factor of 10. The positive outcomes from these discussions paved the way for the negotiation of the Chemical Weapons Convention in the Conference on Disarmament at the United Nations in Geneva. However, as the war progressed and Iraq became more experienced in producing and deploying chemical weapons, Iraq used chemical weapons increasingly as a strategic weapon, including against Iranian non-combatants. In this context, it has been reported by the United Nations that Iraq used more than 1800 tonnes of sulphur mustard, more than 140 tonnes of tabun and more than 600 tonnes of sarin during the Iraq-Iran War. Particularly horrific examples included the use of sulphur mustard against the town of Sardasht in north-western Iran in June 1987, and the use of the nerve agent sarin against 16 | C h a p t e r 1 – I n t r o d u c t i o n a n d h i s t o r i c a l o v e r v i e w the Kurdish village of Halabja in northern Iraq in March 1988 (Figure 1. The large scale use of chemical weapons by Iraq in the Iran-Iraq war in the 1980s was a major driving force for the negotiation of the Chemical Weapons Convention. As a means of overcoming its problems with producing stable nerve agents, Iraq developed a different binary munitions concept, in which the precursors were mixed and the munition filled shortly before it was to be used. The attack killed 13 civilians and seriously injured more than 1,000 others (Figure 1. On 29 April 1997, the Chemical Weapons Convention entered into force, meaning that the prohibition of the production, stockpiling, and use of chemical weapons was finally brought into effect following more than two decades of negotiations in Geneva. The largest scale chemical weapons attack occurred on 21 August 2013, when several opposition-controlled or disputed areas of Ghouta, a suburb of Damascus, were struck by rockets containing sarin. With the destruction of the declared chemical weapons, agent, production and storage facilities, and mixing and filling equipment, Syria’s chemical weapons programme is now largely dismantled. Despite the progress 19 | C h a p t e r 1 – I n t r o d u c t i o n a n d h i s t o r i c a l o v e r v i e w made towards eliminating Syria’s chemical weapons programme, there have been a number of subsequent chemical weapon attacks in Syria using chlorine and other toxic industrial chemicals. Chemical and bacteriological (biological) weapons and the effects of their possible use: report of the Secretary-General. Planning and training of these personnel will be necessary for effective management of such incidents, particularly those involving a large number of chemical casualties whose arrival in surges at a medical support facility is likely to exceed its normalcapacity. Hazard avoidance through adequate protection and decontamination, as well as cordons to control entry to and exit from the affected area;. Casualty decontamination, not only to reduce contact of the agent with the victim, but to avoid spreading contamination to medical treatment facilities; and. Triage and quick medical treatment, including specific antidote therapy at the site of the incident and at the hospital level to reduce morbidity and mortality. It is important to note that medical personnel may have to deal with mass casualties, some of whom may not even have been poisoned but who may have psychogenic symptoms. The plan should clearly integrate medical capabilities at the local, regional, and national levels. This may require the establishment of coordination agreements between different services and agencies so they can be integrated smoothly into the command and control system. Management plans should be as simple as possible and be clearly expressed, as complex plans may be difficult to implement. Such actions might include disposal of hazardous materials and remediation of the incident site, as well as further assistance to victims. Medical management is important in all phases, although often these phases overlap and the duration of each one will vary depending on the nature and severity of the incident. Moreover, results of unambiguous identification from laboratory identification of environmental and clinical samples will take time to reach medical personnel. Fourier transform infrared spectroscopy; 25 | C h a p t e r 2 – G e n e r a l c o n s i d e r a t i o n s. All portable detection/identification devices, regardless of the technology used, sometimes yield false positives and false negatives due to their sensitivity and selectivity. Using detectors with one technology provides “provisional” detection, while using detectors of at least two different technologies provides a higher level of assurance, in particular if a colourimetric method or gas chromatography/mass spectrometry is one of the two techniques used or employed (Figure 2.
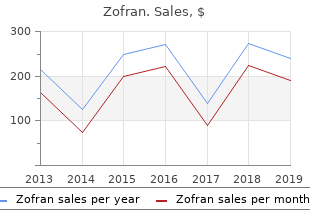
For this reason as well as for comparability medications list template generic 4mg zofran with amex, in the meta-analyses of all studies the outcome at 12 weeks was used symptoms of cheap 4 mg zofran with amex. Dance is becoming more and more popular as complementary form of exercise for pwp and recommended by many Parkinson associations treatment wpw cheap 4mg zofran amex. The most widely used type of dance by pwp is tango, but also ballroom dancing, Irish set dance and salsa classes are used. Dance often incorporates direct practice of walking in the situations that commonly provoke freezing94 the music provides an external rhythm, which can be considered as auditory cueing (6. As dance requires high-level multitasking and progressive motor skill learning, dance is both physically and cognitively challenging94. The reduced movement amplitude in pwp is targeted by aiming for large amplitude movements265;479-484. However, not all pwp may have access to a (physiotherapist-supervised) Tai Chi training group and costs to participate in a Tai Chi class may be problematic. Here however, we present it as a separate type of intervention, as it is not a type of exercise and is provided as a stand-alone intervention by massage therapists. However, if pain in Parkinson’s disease is not medication related, physiotherapeutic intervention may be indicated. The intervention, based on the mechanisms of pain, will include pain education, addressing the infuence of fear on pain and the importance of staying physical active. Inspiratory muscle training aims to improve pulmonary function and perceived dyspnoea50, and expiratory muscle strength training programmes aim to generate adequate respiratory pressure for coughing to clear foreign materials thus protecting the airways354;508. Both techniques sustain characteristics of voice production to enable good communication, as well as preserving respiratory and swallowing functions50;349;354;356;508. Moreover, physiotherapy guidelines recommend routinely monitoring any person with neuromuscular weakness for clinical features of ventilatory problems, and management with assisted cough strategies and ventilatory assistance accordingly509. These assisted cough strategies, including air stacking, glossopharyngeal breathing, manually assisted coughing and mechanical insuffation–exsuffation, have all been demonstrated to be effective in people with neuromuscular weakness510-515. Practice entails repetitive motor execution to improve the fuency of motor skills, either of original motor skills or, through motor learning, of novel motor skills. Automatisation: skilled behaviour requiring minimal cognitive resources, stable over time and resistant to interference, such as in dual tasking 3. Retention: motor skills readily executed after long delays without further practice on the task the ability to carry out complex tasks and negotiate complex environments relies upon automaticity. Automaticity depends on intact basal ganglia function and therefore is increasingly disturbed in pwp. In general, pwp beneft from practice, but require a higher training dose to achieve results comparable with their contemporaries and show more variable clinical benefts521-524. Because the basal ganglia are critical for the automatisation, acquisition of skills may be relatively preserved, but automatisation and retention are less effcient compared to age matched controls485. The ability to learn a novel skill may be preserved by compensation of the basal ganglia dysfunction with activation of other brain structures such as the cerebellum520;525;526. As the potential for learning is believed to diminish over the disease course, the greatest benefts may be gained at the earlier, mild stage (Hoehn and Yahr 2 to 3)483;485;519;527-529. Taking into account general principles for motor learning and using external cues will enhance acquisition, automaticity and retention108;483;485;519;520;530-532. Interventions that aim to improve motor skills and motor learning in pwp include cued functional training (6. However, laboratory experiments have shown that with instruction, pwp without cognitive impairments are able to prioritise walking and reduce attention to a concurrent cognitive task122;537-540. Moreover, laboratory experiments have shown improved dual task gait after dual-task gait training using visual cues541;542, after treadmill training with virtual obstacles543, and using an attentional strategy (focusing on taking big steps) with or without concurrent auditory cue544. During dual-task gait training, pwp aim to improve walking speed and step length, using visual or auditory cues, while simultaneously undertaking a variety of motor or cognitive challenging tasks535;536. The complexity of both the gait and additional task can be increased progressively. Cognitive tasks known to cause gait interference in older people include536: Verbal fuency: for example ask the pwp to name to name cities starting with a specifc letter Discrimination and decision making tasks: for example ask the the pwp to change gait direction to the right when you say yellow and stop walking when you say red Working memory tasks: for example ask the pwp to distract number by three starting at 90 Mental tracking tasks: for example, tell the pwp a story and ask the pwp how many times you use a specifc word Reaction time tasks: 79 European Physiotherapy Guideline for Parkinson’s disease Examples of dual tasks while walking when aiming for functional training include asking the pwp to describe a certain route or how the past weekend was spent, carrying a tray with water flled glasses, closing buttons or picking objects up from the foor536. If the height cannot be adjusted, a chair with the preferred height and with comparable softness of the seat may be used. External cues support the sit-to-stand transfer, such as verbal commands for each step of the transfer or a visual focus point to move towards Medium Improve Task variability.
Zofran 4 mg discount. Guillain-Barre Syndrome Pneumonia & Esophageal Achalasia Testimonial - Day 3 Treatment 3.
In a milder 222 Mirror Movements M form treatment hemorrhoids discount 4 mg zofran mastercard, known as ‘mirror ataxia’ treatment whooping cough buy zofran uk, patients reach in the direction of the object but with increased errors of reach and grasp treatment 20 discount zofran master card, suggesting that visual information is not adequately transformed into a body-centred frame of reference. Cross References Agnosia; Neglect Mirror Apraxia Patients with mirror apraxia presented with an object that can be seen only in a mirror, when asked to reach for the real object will reach for the virtual object in the mirror. They are usually symmetrical and most often seen when using distal muscles of the upper limb. Mirror move ments are frequently present in young children but prevalence decreases with age. Persistence of mirror movements into adult life (‘congenital mirror movements’) is pathological, as is acquisition in adult life. These movements are uncom mon after acquired brain lesions with no relationship to specific anatomical areas. Congenital mirror movements are associated with skeletal developmental abnormalities, especially of the atlanto-occipital region, such as Klippel–Feil syn drome. They are also seen in 85% of patients with X-linked Kallmann syndrome (hypogonadotrophic hypogonadism and anosmia). Acquired mirror movements have been described following thalamic lesions, and in association with spastic paraparesis, extrapyramidal disorders -223 M Mirror Sign (Parkinson’s disease, multiple system atrophy), Friedriech’s ataxia, phenylke tonuria, and affecting hemiparetic limbs following stroke in young children. There is some neurophysiological evidence from patients with X-linked Kallmann syndrome for the existence of an ipsilateral corticospinal pathway, consistent with other evidence that the congenital condition is primarily a disorder of axonal guidance during development. Concurrent activity within ipsilateral and contralateral corticospinal pathways may explain mirroring of movements. Alternatively, a failure of transcallosal inhibition, acquired at the time of myelination of these pathways, may contribute to the genesis of mirror movements. A deficit of sustained attention has also been postulated as the cause of mirror movements. Abnormal cortex–muscle interactions in subjects with X-linked Kallmann’s syndrome and mirror movements. Cross References Anosmia; Attention; Mirror writing; Proprioception; Synkinesia, Synkinesis Mirror Sign the term ‘mirror sign’ has been applied to the phenomenon of misrecognition of self as another when seen in a mirror. This may occur in Alzheimer’s disease and fron totemporal dementia and is associated with impaired cognition, confabulation, and prefrontal dysfunction. It may lead to a patient complaint of an intruder or a stranger living in the house (‘phantom boarder’ syndrome). Failure to rec ognize oneself in a mirror may also be a dissociative symptom, a symptom of depersonalization. Some authors believe ‘the phenomenon of the mirror’ to be an extreme example of prosopagnosia, but other studies have not found an association. Clinical and neuroanatomical correlates of the mirror sign in frontotemporal dementia and Alzheimer’s disease. Cross References Confabulation; Depersonalization; Misidentification syndromes; ‘Picture sign’; Prosopagnosia Mirror Writing As the name implies, mirror writing is a mirror image of normal writing, hence running from right to left, with characters back to front. This may occur sponta neously, apparently more often in left-handers, or in right-handers attempting to write with the left hand following left-sided brain injury. The author Lewis Carroll occasionally wrote mirror letters but these differ from his normal script, unlike the situation with Leonardo whose two scripts are faithful mirror images. Carroll’s letters may thus reflect not an inherent capac ity but a contrivance, designed to amuse children who corresponded with him. The device was also used by the author Arthur Ransome in his 1939 novel Secret Water. Jane Austen wrote one letter (1817) to a young niece in which script runs from right to left but with word order reversed within words. Various neural mechanisms are proposed to explain mirror writing, includ ing bilateral cerebral representation of language, motor programmes, or visual memory traces or engrams. The mechanisms may differ between a true mir ror writer like Leonardo and someone performing the task for amusement like Carroll. The ability to read mirror reversed text as quickly as normally oriented text has been reported in some autistic individuals.
Post-marketing reports of possible distant spread of toxin have been very rarely reported in pediatric patients with co-morbidities medicine clip art purchase genuine zofran, predominantly with cerebral palsy medications not to take with grapefruit discount zofran master card, who received > 8 U/kg symptoms depression discount zofran 8 mg. Extreme caution should be exercised when treating pediatric patients who have significant neurologic debility, dysphagia, or have a recent history of aspiration pneumonia or lung disease. In general, dose selection for an elderly patient should be cautious, usually starting at the lowest recommended dose for the specific indication. However, weakness of adjacent muscles associated with local diffusion and/or injection technique has been reported. Muscle weakness remote to the site of injection and other serious adverse effects. As is expected for any injection procedure, localized pain, inflammation, paresthesia, hypoesthesia, tenderness, swelling/oedema, erythema, localized infection, bleeding and/or bruising have been associated with the injection. Clinical Trial Adverse Drug Reactions Because clinical trials are conducted under very specific conditions the adverse reaction rates observed in the clinical trials may not reflect the rates observed in practice and should not be compared to the rates in the clinical trials of another drug. Adverse drug reaction information from clinical trials is useful for identifying drug-related adverse events and for approximating rates. The frequency is defined as follows: Very Common (≥ 1/10); Common (≥1/100, <1/10). Nervous system disorders Common: Headache, paresthesia Vascular disorders Common: Hot flush Gastrointestinal disorders Common: Nausea Skin and subcutaneous tissue disorders Common: Hyperhidrosis, skin odor abnormal, pruritus, subcutaneous nodule, alopecia Musculoskeletal and connective tissue disorders Common: Pain in extremity General disorders and administration site conditions Very common: Injection site pain Common: Pain, injection site edema, injection site hemorrhage, injection site 14 hypersensitivity, injection site irritation, asthenia Note: increase in non-axillary sweating was reported in 4. Neurogenic Detrusor Overactivity associated with a neurologic condition the table below presents the most frequently reported adverse reactions in double-blind, placebo-controlled studies within 12 weeks of injection for detrusor overactivity associated with a neurologic condition. Among patients who were not catheterizing at baseline prior to treatment, catheterization was initiated in 38. Overactive Bladder the table below presents the most frequently reported adverse reactions in double-blind, placebo-controlled, pivotal Phase 3 studies within 12 weeks of injection for overactive bladder. Events considered to be procedure-related by the investigator reported at any time following initial injection were dysuria (6%) and haematuria (2%). The frequency is defined as follows: Uncommon (≥1/1,000, <1/100); Rare (≥1/10,000, <1/1,000); Very Rare (<1/10,000). Blepharospasm Nervous system disorders Uncommon Dizziness, facial palsy Eye disorders Uncommon Keratitis, ectropion, diplopia, entropion, vision blurred. Very rare Ulcerative keratitis, corneal epithelium defect, corneal perforation Skin and subcutaneous tissue disorder Uncommon Rash General disorders and administration site conditions Uncommon Fatigue Strabismus Eye disorders Uncommon Ocular retrobulbar hemorrhages, eye penetration, Holmes-Adie pupil Rare Vitreous hemorrhage Cervical dystonia Eye disorders Uncommon Diplopia, eyelid ptosis General disorders and administration site conditions Uncommon Pyrexia Focal Spasticity Nervous system disorders Uncommon: Hypoesthesia, headache, paresthesia Vascular disorders Uncommon: Orthostatic hypotension Gastrointestinal disorders Uncommon: Nausea Skin and subcutaneous tissue disorders Uncommon: Dermatitis, pruritis, rash Musculoskeletal and connective tissue disorders Uncommon: Arthralgia, bursitis 18 General disorders and administration site conditions Uncommon: Asthenia, pain, injection site hypersensitivity, malaise Chronic Migraine Gastrointestinal disorders Uncommon: Dysphagia Skin and subcutaneous tissue disorders Uncommon: Pain of skin Musculoskeletal and connective tissue disorders Uncommon: Pain in jaw Abnormal Hematologic and Clinical Chemistry Findings No specific trends in abnormal hematologic or clinical chemistry findings have been reported. Adverse events after treatment with botulinum toxin include rare spontaneous reports of death, sometimes associated with dysphagia, respiratory compromise, pneumonia, and/or other significant debility. Some of these patients had risk factors including pre-existing cardiovascular disease. The reports in children were predominantly from cerebral palsy patients treated for spasticity. Drug-Drug Interactions Table 1: Established or Potential Drug-Drug Interactions Proper name of drug Ref Effect Clinical comment the effect of botulinum toxin may be aminoglycoside antibiotics or T Theoretically, potentiated by aminoglycoside antibiotics or spectinomycin, or other medicinal the effect of spectinomycin, or other drugs that interfere products that interfere with botulinum with neuromuscular transmission. The effect of administering different botulinum Different botulinum neurotoxin T Unknown neurotoxin serotypes at the same time or within serotypes several months of each other is unknown. Excessive weakness may be exacerbated by administration of another botulinum toxin prior to the resolution of the effects of a previously administered botulinum toxin. Drug-Laboratory Interactions Interactions with laboratory tests have not been established. The exact dosage and number of injection sites should be tailored to the patient’s needs based on the size, number and location of muscles involved, the severity of disease, presence of local muscle weakness, response to previous treatment, and the patient’s medical condition. This dose can be gradually increased in subsequent treatments to the maximum recommended dose, if needed. In treating adult patients, when combining indications, the maximum cumulative dose in a 3 month interval should generally not exceed 6 Units/kg, or 360 Units, whichever is lower. In treating pediatric patients, the maximum cumulative dose in a 3 month interval should generally not exceed 6 Units/kg body weight, or 200 Units, whichever is lower.