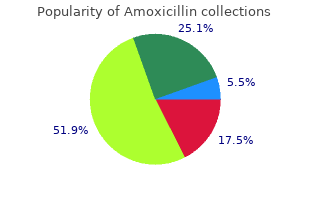
Amoxicillin
"Purchase amoxicillin from india, medications ok for pregnancy."
By: Connie Watkins Bales, PhD
- Professor in Medicine
- Senior Fellow in the Center for the Study of Aging and Human Development

https://medicine.duke.edu/faculty/connie-watkins-bales-phd
Pit-1 also binds to the prolactin gene in multiple sites in both the promoter region and in an adjacent region symptoms low potassium buy amoxicillin 250 mg with visa, designated as a distal enhancer; Pit-1 binding is a requirement for prolactin promoter activity and gene transcription medicine 029 amoxicillin 250 mg low cost. Many hormones medications like prozac buy cheap amoxicillin 250mg online, neurotransmitters, and growth factors influence the prolactin gene, involved in a level of function beyond that allowed by Pit-1. Fundamental modulation of prolactin secretion is exerted by estrogen, 18, 19 producing both differentiation of lactotrophs and direct stimulation of prolactin production. An estrogen response element is adjacent to one of the Pit-1 binding sites in the distal enhancer region, and estrogen stimulation of the prolactin gene involves interaction with this Pit-1 binding site. Estrogen also influences prolactin 20 production by suppressing dopamine secretion. Surfactant synthesis in the fetal lung is influenced by prolactin, and decidual prolactin modulates 21, 22 prostaglandin-mediated uterine muscle contractility. Prolactin also contributes to the prevention of the immunologic rejection of the conceptus by suppressing the maternal immune response. The mechanisms and purpose for mammary production of prolactin remain to be determined, but prolactin in milk is believed to be derived from local synthesis. Transmission of this prolactin to the newborn may be important for immune functions. Dopamine is secreted by the basal hypothalamus into the portal system and conducted to the anterior pituitary. Dopamine binds specifically to lactotroph cells and suppresses the secretion of prolactin into the general circulation; in its absence, prolactin is secreted. Dopamine binds to a G protein-coupled receptor ( Chapter 2) that exists in a long form and a short form, but only the D2 (long form) is present on lactotrophs. However, except in hypothyroidism, normal physiologic changes as well as abnormal prolactin secretion are easily explained and understood in terms of variations in the prolactin inhibiting factor, dopamine. A large collection of peptides has been reported to stimulate the release of prolactin in vitro. But it is unknown whether these peptides participate in the normal physiologic regulation of prolactin secretion. The Prolactin Receptor the prolactin receptor is encoded by a gene on chromosome 5p13–14 that is near the gene for the growth hormone receptor. The prolactin receptor belongs to a 25 receptor family that includes many cytokines and some growth factors, supporting a dual role for prolactin as a classic hormone and as a cytokine. Prolactin receptors exist in more than one form, all containing an extracellular region, a single transmembrane region, and a relatively long cytoplasmic domain. There 26 is evidence for more than one receptor, depending upon the site of action . The amino acid identity between prolactin and growth 27 hormone receptors is approximately 30%, with certain regions having up to 70% homology. A protein also exists that functions as a receptor/transporter, translocating prolactin from the blood into the cerebrospinal fluid, the amniotic fluid, and milk. Amniotic Fluid Prolactin Amniotic fluid concentrations of prolactin parallel maternal serum concentrations until the 10th week of pregnancy, rise markedly until the 20th week, and then decrease. Indeed, the source of amniotic fluid prolactin is neither the maternal pituitary nor the fetal pituitary. The failure of dopamine agonist treatment to suppress amniotic fluid prolactin levels, and studies with in vitro culture systems, indicate a primary decidual source with transfer via amnion receptors to the amniotic fluid, requiring the intactness of amnion, chorion, and adherent decidua. This decidual synthesis of 28 prolactin is initiated by progesterone, but once decidualization is established, prolactin secretion continues in the absence of both progesterone and estradiol. Various decidual factors regulate prolactin synthesis and release, including relaxin, insulin, and insulin-like growth factor-I (discussed in Chapter 4). However, the amino acid sequence and the chemical and biological properties of decidual prolactin are identical to those of pituitary prolactin. It is hypothesized that amniotic fluid prolactin plays a role in modulating electrolyte economy not unlike its ability to regulate sodium transport and water movement across the gills in fish (allowing the ocean-dwelling salmon and steelhead to return to freshwater streams for reproduction). Thus prolactin would protect the human fetus from dehydration by control of salt and water transport across the amnion. Prolactin reduces the permeability of the human amnion in the fetal to maternal direction by 29 a receptor-mediated action on the epithelium lining the fetal surface. Lactation During pregnancy, prolactin levels rise from the normal level of 10–25 ng/mL to high concentrations, beginning about 8 weeks and reaching a peak of 200–400 ng/mL 30, 31 at term.
Noci I symptoms 24 hour flu generic 500 mg amoxicillin overnight delivery, Biagiotti R symptoms 5-6 weeks pregnant buy cheap amoxicillin 250mg on-line, Maggi M medicine wheel images purchase amoxicillin with paypal, Ricci F, Cinotti A, Scarselli G, Low day 3 luteinizing hormone values are predictive of reduced response to ovarian stimulation, Hum Reprod 13:531, 1998. Homburg R, Levy T, Ben-Rafael Z, A comparative prospective study of conventional regimen with chronic low-dose administration of follicle-stimulating hormone for anovulation associated with polycystic ovary syndrome, Fertil Steril 63:729, 1995. Leerentueld R, Van Gent I, Der Stoep M, Wladimiroff J, Ultrasonographic assessment of Graffian follicle growth under monofollicular and multifollicular conditions in clomiphene citrate stimulated cycles, Fertil Steril 43:565, 1985. Tal J, Paz B, Samberg I, Lazarov N, Sharf M, Ultrasonographic and clinical correlates of menotropin versus sequential clomiphene citrate: menotropin therapy for induction of ovulation, Fertil Steril 44:342, 1985. Nakamura Y, Yoshimura Y, Yamada H, Ubukata Y, Yoshida K, Tamaoka Y, Suzuki M, Clinical experience in the induction of ovulation and pregnancy with pulsatile subcutaneous administration of human menopausal gonadotropin: a low incidence of multiple pregnancy, Fertil Steril 51:423, 1989. Ho Yuen B, Pride S, Induction of ovulation with exogenous gonadotropins in anovulatory infertile women, Seminars Reprod Endocrinol 8:1861, 1990. Fernandez H, Coste J, Job-Spira N, Controlled ovarian hyperstimulation as a risk factor for ectopic pregnancy, Obstet Gynecol 78:656, 1991. Hamilton-Fairley D, Kiddy D, Watson H, Paterson C, Franks S, Association of moderate obesity with a poor pregnancy outcome in women with polycystic ovary syndrome treated with low dose gonadotropin, Br J Obstet Gynaecol 99:128, 1992. Corchia C, Mastroiacovo P, Lanni R, Mannazzu R, Curro V, Fabris C, What proportion of multiple births are due to ovulation induction? Derom C, Derom R, Vlietink R, Van Den Berghe H, Thiery M, Increased monozygotic twinning rate after ovulation induction, Lancet i:1236, 1987. Bohrer M, Kemmann E, Risk factors for spontaneous abortion in menotropin-treated women, Fertil Steril 48:571, 1987. Kol S, Levron J, Lewit N, Drugan A, Itskovitz-Eldor J, the natural history of multiple pregnancies after assisted reproduction: is spontaneous fetal demise a clinically significant phenomenon? Mashiach S, Bider D, Moran O, Goldenberg M, Ben-Rafael Z, Adnexal torsion of hyperstimulated ovaries in pregnancies after gonadotropin therapy, Fertil Steril 53:76, 1990. Neulen J, Yan Z, Raczek S, Weindel K, Keck C, Weich Ha, Marme D, Breckwoldt M, Human chorionic gonadotropin-dependent expression of vascular endothelial growth factor/vascular permeability factor in human granulosa cells: importance in ovarian hyperstimulation syndrome, J Clin Endocrinol Metab 80:1967, 1995. Rizk B, Aboulghar M, Modern management of ovarian hyperstimulation syndrome, Hum Reprod 6:1082, 1991. Fournet N, Surrey E, Kerin J, Internal jugular vein thrombosis after ovulation induction with gonadotropins, Fertil Steril 56:354, 1991. Zosmer A, Katz Z, Lancet M, Konichezky S, Schwartz-Shoham Z, Adult respiratory distress syndrome complicating ovarian hyperstimulation syndrome, Fertil Steril 47:524, 1987. Fakih H, Bello S, Ovarian cyst aspiration: a therapeutic approach to ovarian hyperstimulation syndrome, Fertil Steril 58:829, 1992. McNaughton J, Banah M, McCloud P, Hee J, Burger H, Age related changes in follicle stimulating hormone, luteinizing hormone, oestradiol and immunoreactive inhibin in women of reproductive age, Clin Endocrinol 36:339, 1992. Farhi J, Homburg R, Ferber A, Orvieto R, Ben Rafael Z, Non-response to ovarian stimulation in normogonadotrophic, normogonadal women: a clinical sign of impending onset of ovarian failure pre-empting the rise in basal follicle stimulating hormone levels, Hum Reprod 12:241, 1997. Homburg R, Levy T, Berkovitz D, Farchi J, Feldberg D, Ashkenazi J, Ben-Rafael Z, Gonadotropin-releasing hormone agonist reduces the miscarriage rate for pregnancies achieved in women with polycystic ovarian syndrome, Fertil Steril 59:527, 1993. Mizunuma H, Andoh K, Yamada K, Takagi T, Kamijo T, Ibuki Y, Prediction and prevention of ovarian hyperstimulation by monitoring endogenous luteinizing hormone release during purified follicle-stimulating hormone therapy, Fertil Steril 58:46, 1992. Devroey P, Mannaerts B, Smitz J, Coelingh Bennink H, Van Steirteghem A, Clinical outcome of a pilot efficacy study on recombinant human follicle-stimulating hormone (Org 32489) combined with various gonadotrophin-releasing hormone agonist regimens, Hum Reprod 9:1064, 1994. Levy T, Limor R, Villa Y, Eshel A, Eckstein N, Vagman I, Lidor A, Ayalon D, Another look at co-treatment with growth hormone and human menopausal gonadotrophins in poor ovarian responders, Hum Reprod 8:834, 1993. Tulandi T, Galcone T, Guyda H, Hemmings R, Billiar R, Morris D, Effects of synthetic growth hormone-releasing factor in women treated with gonadotrophin, Hum Reprod 8:525, 1993. Filicori M, Flamigni C, Dellai P, Cognigni G, Michelacci L, Arnone R, Sambataro M, Falbo A, Treatment of anovulation with pulsatile gonadotropin-releasing hormone: prognostic factors and clinical results in 600 cycles, J Clin Endocrinol Metab 79:1215, 1994. Kovacs G, Buckler H, Gangah M, Burger H, Healy D, Baker G, Phillips S, Treatment of anovulation due to polycystic ovarian syndrome by laparoscopic ovarian electrocautery, Br J Obstet Gynaecol 98:30, 1991. Campo S, Ovulatory cycles, pregnancy outcome and complications after surgical treatment of polycystic ovary syndrome, Obstet Gynecol Survey 53:297, 1998. Campo S, Ovulatory cycles, pregnancy outcome and complications after surgical treatment of polycystic ovary syndrome, Obstet Gynecol Survey 53:297, 1998. Simon A, Laufer N, Unexplained infertility: a reappraisal, Assist Reprod Rev 3:26, 1993. Karlstrom P-O, Bergh T, Lundkvist O, A prospective randomized trial of artificial insemination versus intercourse in cycles stimulated with human menopausal gonadotropin or clomiphene citrate, Fertil Steril 59:554, 1993. Fujii S, Fukui A, Fukushi Y, Kagiya A, Sato S, Saito Y, the effects of clomiphene citrate on normal ovulatory women, Fertil Steril 68:997, 1997.
Review the side effects that can affect continuation: amenorrhea symptoms e coli generic amoxicillin 500 mg mastercard, breakthrough bleeding symptoms 9 days post ovulation order amoxicillin toronto, headaches treatment 12th rib syndrome discount amoxicillin 250 mg on-line, weight gain, nausea, etc. Explain the warning signs of potential problems: abdominal or chest pain, trouble breathing, severe headaches, visual problems, leg pain or swelling. Ask the patient to be sure to call if another clinician prescribes other medications. Ask the patient to repeat critical information to make sure she understands what has been said. Schedule a return appointment in 1–2 months to review understanding and address fears and concerns; a visit at 3 months is too late because most questions 343 341 and side effects occur early. Inconsistent use of oral contraceptives is more common in women who are new starters. Ask the patient to call for any problem or concern before she stops taking the oral contraceptives. The Progestin-Only Minipill 345, 346 the minipill contains a small dose of a progestational agent and must be taken daily, in a continuous fashion. There is no evidence for any difference in clinical behavior among the available minipill products. Mechanism of Action After taking a progestin-only minipill, the small amount of progestin in the circulation (about 25% of that in combined oral contraceptives) will have a significant impact only on those tissues very sensitive to the female sex steroids, estrogen and progesterone. The contraceptive effect is more dependent upon endometrial and cervical mucus effects, because gonadotropins are not consistently suppressed. The endometrium involutes and becomes hostile to implantation, and the cervical mucus becomes thick and impermeable. Because of the low dose, the minipill must be taken every day at the same time of day. The change in the cervical mucus requires 2–4 hours to take effect, and, most importantly, the impermeability diminishes 22 hours after administration, and by 24 hours sperm penetration is essentially unimpaired. Although the overall incidence of ectopic pregnancy is not increased (it is still much lower than the incidence in women not using a contraceptive method), when pregnancy occurs, the clinician must suspect that it is more likely to be ectopic. A previous ectopic pregnancy should not be regarded as a contraindication to the minipill. Only one disturbing observation has been reported; progestin-only oral contraception was associated with about a 3-fold incrased risk of diabetes mellitus in lactating women with recent gestational diabetes (an observation that is difficult 130 to explain). Because this increased risk is not observed with the use of combined oral contraceptives, it is speculated that the low levels of estrogen associated with breastfeeding allow an unimpeded progestin effect on insulin resistance. In motivated women, the failure rate is comparable to the rate (less than 1 per 100 350, 351 and 352 woman-years) with combination oral contraception. Pill Taking the minipill should be started on the first day of menses, and a backup method must be used for the first 7 days because some women (very few) ovulate as early as 7–9 days after the onset of menses. The pill should be keyed to a daily event to ensure regular administration at the same time of the day. If pills are forgotten or gastrointestinal illness impairs absorption, the minipill should be resumed as soon as possible, and a back-up method should be used immediately and until the pills have been resumed for at least 2 days. If 2 or more pills are missed in a row and there is no menstrual bleeding in 4–6 weeks, a pregnancy test should be obtained. If more than 3 hours late in taking a pill, a backup method should be used for 48 hours. Problems In view of the unpredictable effect on ovulation, it is not surprising that irregular menstrual bleeding is the major clinical problem. The daily progestational impact on the endometrium also contributes to this problem. Patients can expect to have normal, ovulatory cycles (40%), short, irregular cycles (40%), or a total lack of cycles 352 ranging from irregular bleeding to spotting and amenorrhea (20%). This is the major reason why women discontinue the minipill method of contraception. Women who have experienced frequent ovarian cysts would be happier with methods that effectively suppress ovulation (combined oral contraceptives and depot-medroxyprogesterone acetate). Therefore free steroid levels (levonorgestrel and testosterone) will be increased despite the low dose. The incidence of the other minor side effects is very low, probably at the same rate that would be encountered with a placebo.
Existing systematic reviews compare mechanical with bioprosthetic valves in the aortic or mitral and tricuspid position symptoms webmd buy amoxicillin 500 mg, but all of these reviews have important methodological limitations that may bias results treatment wpw order on line amoxicillin. A recent high-quality review compared stented with stentless bioprosthetic valves and found mixed short- term hemodynamic benefits for stentless valves treatment yeast in urine buy 250 mg amoxicillin with visa, but with the tradeoff of longer cross-clamp and 35 heart-lung bypass times. Only one review compared two different stented bioprosthetic 39 valves, and we did not identify any systematic reviews comparing differing mechanical valves. Surgical and anesthetic techniques have improved over time, potentially confounding comparisons across time periods. Valve designs have also changed over time, and those changes are not always reliably reflected by changes to valve names; moreover, valve names are not reported in a uniform manner, complicating accurate valve classification. Percutaneous heart valves have been developed and evaluated by at least seven companies. Some of these valves are approved for use in Europe, and most of the published literature originates from this region. The peer-reviewed literature describes just over 900 patients, assessed as being at high risk for conventional valve replacement, who have received these valves. The first percutaneous heart valve replacement procedures were conducted by accessing the venous system via the femoral vein and passing a catheter through the septum of the heart to reach (and traverse) that aortic valve. This antegrade approach via the femoral vein now appears to have been replaced by one of two emerging approaches: (1) a retrograde approach via the femoral artery; or (2) a transapical approach via the apex of the heart. Three other retrograde approaches—via the subclavian or axillary artery or the ascending aorta—have also been reported. Unlike the antegrade approach via the femoral vein, retrograde approaches do not require perforating and traversing the cardiac septum but present important technical challenges, in large part because of the calcified and tortuous arteries that must be navigated with a relatively large catheter. In contrast, the more recently developed transapical approach obviates the need 29 for maneuvering a catheter through either arteries or veins, but it requires making an incision in the chest wall and traversing the myocardium. All six percutaneous approaches reported in the published literature may require some additional training of cardiac surgeons or interventional cardiologists, as well as some modifications to existing catheter labs or operating suites. To date, few groups in the United States have significant experience with percutaneous heart valve replacement. Although the initial experience demonstrates that percutaneous heart valves can be implanted with good short- term success, longer term survival, valve durability, and complication rates are unknown. Even comparison of short-term success to historical controls is problematic because predicted mortality is based on imperfect risk prediction models that were developed for other cardiac surgeries. A further limitation of the extant literature is the subjective nature of patient selection as “too high risk for surgery,” making appropriate patient selection less certain. Future Research the long-term durability of mechanical heart valves is well established and has been shown to be superior to that of early generation bioprosthetic valves. Since bioprosthetic valves do not require chronic anticoagulation, durability is a critical issue in determining at what age to recommend them instead of mechanical valves. An updated review may also be able to evaluate specific valves within each class, including currently marketed newer vs. Because the number of direct comparisons is limited for many valves and some valve classes, indirect comparisons using network meta- analysis may be useful. What are the complication rates, durability, and effects on mortality and health-related quality of life? How do these valves compare with conventional valve replacement in lower risk patients? Which procedural and setting factors, including procedural volume, are related to clinical outcomes? How do discharge rates to extended care facilities, rates of rehospitalization after valve placement, and changes in functional status compare to other treatment options? We identified specific opportunities for improved reporting that would facilitate comparative effectiveness studies. Standardized reporting of methods and outcomes of 30 percutaneous heart valve replacement is especially important in light of the evolution of this technology.
Having confidence in the differentiation of these two findings will expedite appropriate progression of care symptoms sleep apnea purchase 250 mg amoxicillin mastercard. Lesion Type T1 T2 T2 with Fat suppression Hemangioma Bright Bright Dark Metastasis Dark Bright Bright Figure 14:5 symptoms 0f high blood pressure purchase 500 mg amoxicillin overnight delivery. Some images tend to have more pronounced variations of this normal anatomical finding medications journal cheap 250mg amoxicillin with mastercard. Prominent basivertebral veins are normal variants that may draw attention from an untrained eye. Prominent appearance of the basivertebral veins at every level in this T2W sagittal image. Clinical imaging: with skeletal, chest and abdomen pattern differentials(third edition). Vertebral abnormality in a patient with suspected malignancy Proc (Bayl Univ Med Cent). Anchoring or tethering the nerve roots or the cord into a position of lesion is one of the most disturbing aspects of a conjoined nerve root. Though most conjoined nerve roots will not be symptomatic, symptoms may develop if the conjoined nerve tethers a nerve root into the path of a herniation, stenosis, or other compressive lesion. The nerve roots normally exit the intervertebral foramina in the upper 1/3 of the foramina. If a conjoined nerve tethers a nerve root so that it exits the lower portion of the foramina, it will be much more susceptible to the pressure of a disc herniation, facet hypertrophy, or foraminal stenosis. This can create a clinically significant complex for manual practitioners, surgeons, therapists, and pain practitioners. Therefore, relying on clues from axial and sagittal images is the best Figure 15:1. Figure 15:3 shows a group of several rootlets grouped together on the left side of the central canal (circled in red). T2W axial image showing two nerves sharing the same anterior sacral foramina (red circle). T2W sagittal image and schematic showing an anchoring of the L5 nerve root in the lower portion of the L5-S1 foramina (red circle). Note that all of the other nerve roots exit through the upper 1/3 of the lumbar intervertebral foramina (yellow arrows). This location prevents the nerve from being too vulnerable to compression from disc bulges, herniations and degenerative hypertrophy. T2W sagittal image and schematic showing an anchoring of the L4 nerve root in the lower portion of the L4-L5 foramina. This condition is hard to diagnose and frequently is missed by radiologists and clinicians. There also seems to be an increased rate of conjoined nerve roots in patients with other vertebral malformations. These conditions include spina bifida, spondylolisthesis, and other posterior vertebral defects. Conjoined lumbar nerve roots: A frequently underappreciated congenital abnormality. Journal of Spinal Disorders & Techniques: April 2004 - Volume 17 - Issue 2 - pp 86-93. Clinical features of conjoined lumbosacral nerve roots versus lumbar intervertebral disc herniations Eur Spine J. Developmental asymmetry of roots of the cauda equina at metrizamide myelography: report of seven cases with a review of the literature. Spinal cord lesions fall into one of three categories: extradural, extramedullary, and intramedullary. Extradural lesions are spinal lesions found in the spine, but outside of the thecal sac.
500 mg amoxicillin for sale. Dehydration signs in Children | Subh Savaray Pakistan | 14 March 2019 | 92NewsHD.